Years ago in the news business, a measure of success in the digital world was page views. We all wanted them and measured success based on how many we got.
The page view obsession eventually wore out as we realized this: It was kind of a phony measurement, mainly because we could drive that number with sensational or even salacious content that would appeal to non-local audiences. That in turn, brought traffic to advertisers that didn’t really do the businesses any good.
For example, if in Tallahassee we ran across the story of a three-headed alligator that was eating family pet kittens, that would draw readers from across the globe. But if I’m a local bank or furniture store buying ads on the web site, what good do those eyeballs do for my business?
So we moved on to other more relevant metrics, which wasn’t to say we ignored page views. Local page views are great! But we also wanted to see how long readers stayed on site and how often they returned and stuff like that. That is, we wanted the most relevant info we could find.
I’m suggesting today that COVID “cases” are the page views of the pandemic.
Again, that’s not to say they are irrelevant, but they are not the most useful metric to measure the impact of this deadly, dreaded virus.
This is an important issue to consider as schools start back up and with the backdrop of our local university settings.
Here are the reasons I don’t think cases are the best measure of the impact of the virus:
- Not all cases are created equal
- Contracting the virus isn’t the worst case — being hospitalized or dying from it is
- Cases are tied to testing which we know is imperfect, inconsistently administered and evolving.
Let’s start with “not all cases are created equal.”
According to the Florida Dept. of Health, the state has had just under 50,000 children (ages 17 and under) diagnosed with COVID-19, through Aug. 26. Florida, also as of the 26th, had about 659,000 total cases. That’s 7.6 percent of cases. But under 18-year-olds make up almost 20 percent of the population, according to the U.S. census, so clearly COVID is weighted away from young people in terms of number of cases (at least the ones that have been tested).
But what about severity?
Let’s compare young people to the oldest segments of our population.
And let’s go national so we don’t get any demographic wonkiness Florida might add to the mix.

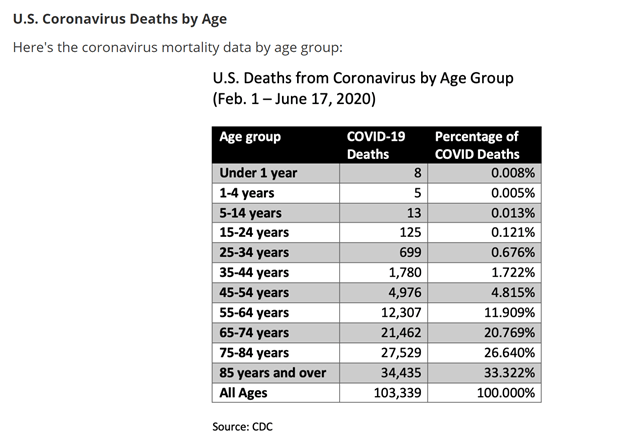
In the U.S., those 17 and under have made up 8.1 percent of the cases, while those 75 and over have made up almost the exact same amount — 7.9 percent. That’s according to the CDC.
But when it comes to the share of fatalities, a total of 85 Americans in the under 17 age bracket have died — out of the 150,000-plus total — that’s six hundreths of one percent of the total fatalities. For those over 75, almost 79,000 have died, which is 58 percent of the fatalities.
(And let’s just stop right there and say that some of the “they were going to die soon anyway” rationalizations for all those elderly deaths are disgusting. Even if an elderly life is cut short by three months, it’s a tragedy. I’m not diminishing elderly deaths AT ALL. Rather, I am showing how the threat to the elderly compares and how measuring cases can distort the view of how the pandemic is affecting any given community).
Let’s put those numbers another way.
If you divide the number of fatalities into the number of cases for those 75 and older, you get a fatality every 4.3 cases, or a 23 percent fatality rate for cases. For those under 17, it’s a fatality every 4,100 cases or a .02 percent fatality rate.
Here’s the number I’ve been trying to get to. By dividing 4.3 into 4,1000, I get it:
It takes 953 cases in someone under 17 to equal just ONE case in someone 75 or older, when it comes to the risk of fatality.
So, when you see that Florida added X thousand cases in a day — what was the median age of those cases?
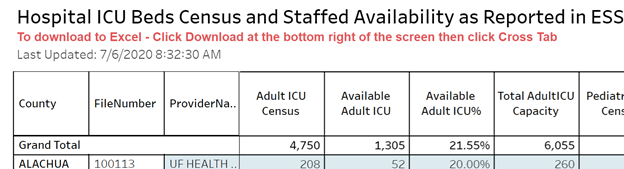
One reason Leon County’s fatality rate has been so low is that the median age of a case is 29. Compare that to Charlotte County (lots of retirees) where the median age of a case is 54. Charlotte County has had 110 deaths out of about 2,600 cases. Leon: 33 deaths out of about 6,200 cases.
Here’s the other thing I don’t think we fully recognize and grasp as a society.
Lots and lots of people die every year and more of them are young than we would ever want to imagine.
Here is a chart of U.S. annual deaths for 2020 (actually, starts Feb. 1, which is I guess when COVID data starting flowing, but you get the idea) from COVID and all other causes from the CDC.
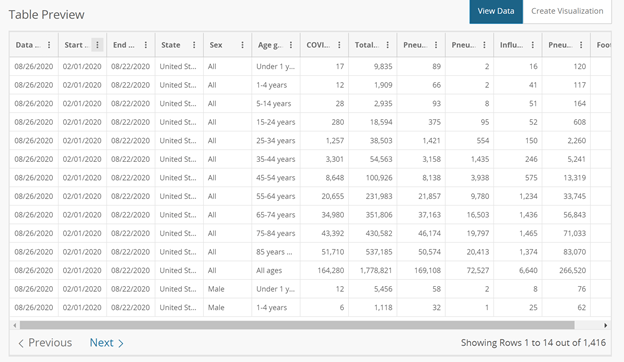
I guess I’ve never really thought about the fact that millions of people die every year in America.
What’s really surprising is the 15,000 or so people ages 14 and under who have died this year of all causes. As you can see, COVID victims make up just .3 percent of all deaths in that age range. Even in those over 85, COVID has made up less than 10 percent of all fatalities. (Yes, I know there are disputes about the data and how things are coded — I hear from both sides that the numbers are fudged higher or lower to help one side of the other. Frankly, I don’t think either side is smart enough to pull off that kind of a conspiracy).
So, what’s my point?
First of all, looking at cases is one of the worst metrics to use when analyzing the impact of the virus.
Hospitalizations are a clear signal of a severe case and, of course, death is the ultimate price to pay for contracting COVID.
One telling fact here is from the University of Alabama, which has garnered national headlines recently for COVID outbreaks. More than 1,000 University of Alabama students have COVID-19.
Of those, do you know how many have been hospitalized? Zero. Now, given the delay from the onset of symptoms to hospitalization, that number may or may not start moving.
As an aside, here is a question: Why in the world would you want to send infected college students home, where they interact with all sorts of more vulnerable people while traveling and then while back in their home communities? In a dorm, they are just passing around COVID to a group of people with just a tiny risk of having a severe impact from the disease (I had somebody in health care tell me recently that FSU’s campus will be the safest place in the world by November because it will have achieved its own little “herd immunity”).
This is also why five Notre Dame professors penned a public letter urging the administration to keep on-campus learning, which the university ultimately did.
Second, when looking at the big picture, the risk for young people when it comes to COVID remains very, very small.
Here are the 10 leading causes of death for young people, from a New England Journal of Medicine study in 2018.
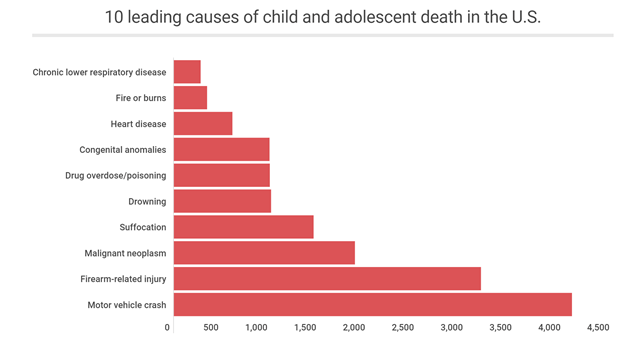
Even if COVID death numbers for this age group (19 and under) more than doubles the rest of this year to almost 200, COVID-19 wouldn’t even make the top 10 causes of death for young people (chronic lower respiratory disease took 274 lives in 2018).
On the other hand (a clause you will read a lot on this site), there is still much we don’t know about how the virus affects people, including the possibility of myocarditis (weakness of heart muscle) and possible neurological impacts.
My third point — if you think this is an attempt to oversimplify the issue of attending school or the like, I refer you back to earlier blog postings.
This is still incredibly complicated.
There is still the issue of young people infecting older more vulnerable people. There are still tough questions about how students interact with teachers, school staff and others on campus. And even within the young people cohort are individuals who are at higher risk than their peers, because of underlying health conditions or other factors.
No, this isn’t simple. But that cuts both ways. Merely pointing at case numbers and declaring that being in school is unsafe is also oversimplifying the situation.
And on the other end of the spectrum — what are we doing to protect those elderly Americans who are at such a scarily vulnerable place with COVID?
Finally, you’ll notice there is no politics in here — there are plenty of places you can go to have that conversation. I’m just interested in data and what conclusions and inferences can be drawn from that data. And by the way, lest you think I’m a complete idiot, I’ve had this piece and those like it reviewed by a journalist, two health care professionals as well as the toughest judges of all — family members — pre-posting.
Feel free to chime in with your views, of course. But if you are going to take this down a political path, you are unlikely to get engagement from me on that — I’ll probably only give you a page view.